In healthcare and long-term care settings, falls are one of the most common accidents.
They are especially common among older adults, and in some cases, a fall can lead to a fracture, trigger a decline that leaves a person bedridden, and significantly affect their quality of life (QOL).
For staff as well, responding after a fall places a heavy burden on daily care, so preventing falls as much as possible is always an important goal.
Various fall-prevention measures are already used in care settings.
However, staff cannot stay beside each person and monitor them at all times.
In recent years, staffing shortages have made technologies that support monitoring, such as sensor-based systems, feel even more important.
One such system that caught my attention in the Silver Industry Newspaper was aams+, a product that not only detects vital signs but also uses AI to notify staff of fall risk.
So how does aams+ actually make this kind of “fall risk notification” possible?
In this article, I will look at fall risk from the perspective of actual care settings, explain how sensors collect biometric data, and examine how aams+ evaluates fall risk, including related patent information.
I will also consider how this kind of system may be used in practice.
Please note that this article is based on my personal views and research.
It does not guarantee the accuracy of the information provided.
Any decision to purchase or use the products introduced here should be made at your own discretion and responsibility.
- Factors That Affect Fall Risk
- aams+
- Practical Use in Care Settings
- It May Reduce the Burden of Room Rounds
- It May Support More Individualized Care by Making Sleep Patterns Visible
- The Displayed Fall Risk Should Be Treated as a Starting Point, Not the Final Judgment
- It May Also Be Helpful in End-of-Life Care or Sudden Changes in Condition
- Recorded Data May Also Help When Consulting Physicians
- Sensors Alone Cannot Capture Everything Related to Fall Risk
- Points to Consider Before Introducing the System
- Closing thoughts
- References
Factors That Affect Fall Risk
A Person’s Ability to Move
Fall risk is influenced not only by physical factors such as disease, muscle strength, balance, joint range of motion, and vision, but also by reduced consciousness or cognitive decline.
When these are affected, a person may no longer be able to respond appropriately to avoid falling.
A Person’s Intention to Move, and the Frequency and Timing of Movement
People do not move only because they have a specific task to do, such as going to the toilet. Emotional factors, including anxiety or pain, may also trigger movement.
In addition, delirium, which is a temporary disturbance in awareness, and cognitive decline can lead to behavior at unexpected times.
And when the frequency and timing of movement change, fall risk can also change significantly.
Environmental Factors
The surrounding environment is also directly linked to fall risk.
This includes the height of the bed, obstacles, footwear, clothing, lighting, handrails, how slippery the floor is, and even the distance to the nurse call button.
Falls Often Occur When Multiple Factors Overlap
In many cases, falls happen when these factors overlap.
One issue that is especially common among older adults is the gap between their actual physical ability and how they perceive their own ability.
When a person does not fully understand or accept the decline in their physical function, they may still believe, “I can do this,” and attempt to move on their own, which can lead to a fall.
In people with dementia, the risk becomes even higher.
It may be difficult not only for them to recognize this gap, but also to understand their surroundings and the situation they are in.
aams+
What Is aams+?
aams is a mat- or sheet-type monitoring system provided by Biosilver Co., Ltd.
By placing it under a bed mattress, the system can display the user’s heart rate, respiration, body movement, bed-exit status, and other conditions in real time, and it alerts staff when something unusual occurs.
The version introduced here, aams+, is a monitoring robot that combines this conventional real-time monitoring function with AI-based fall prediction.
It identifies the people who need closer observation and helps improve the efficiency of monitoring tasks.
Features
- It uses a sensor that works simply by being placed under the mattress, so there is no need for the user to wear or attach anything.
- It can display heart rate, respiration, body movement, bed-exit status, sleep, and similar information on a monitor in real time.
- It is equipped with Reha3.0, a fall prediction system developed by Rehabilitation3.0. Based on the heart rate, respiration, and sleep data collected by aams, as well as day-to-day changes in that data, it estimates “motor ability” and “cognitive ability,” then predicts each morning which individuals are at high risk of falling that day.
The results are displayed in three levels: High Risk, Caution, and Attention Required. - In addition to alerts for unusual changes, it can also be linked to a nurse call system.
- It can store data histories and integrate with care record software.
- It has obtained a TAIS code and the “Care Technology” mark, and its product information is registered in the Techno-Aids Association database, which may make it easier for the product to qualify for subsidies.
How It Works
Key Points of aams+
According to the official website, the basic process behind aams+ can be summarized as follows:
- A mat-type sensor collects vital data
- ADL indicators (FIM) are automatically estimated
- Based on those results, fall risk is classified into three levels—High Risk, Caution, and Attention Required—and the risk status of all residents is displayed in a list
At this time, I was not able to find a patent specifically for aams itself.
However, based on related patents and other available information, I will look at how steps 1 through 3 may work.
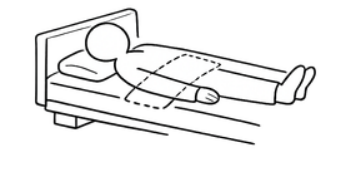
1) How the Mat-Type Sensor Works
First, let us look at step 1: how aams+ collects information from a person lying in bed simply by placing a mat under the mattress.
Since I could not find a patent application specifically for aams+ itself, I will refer here to a related patent for Suishin Delta, a product by Health Sensing Co., Ltd. that also uses a mat- or sheet-type sensor to collect biometric data.
(Patent No. 7301275)
In general, accurate evaluation of sleep usually requires polysomnography, in which sensors are attached to the head, chest, and other parts of the body.
However, Suishin Delta is designed to obtain information about sleep status simply by having a person lie on top of a sheet-type sensor.
The system extracts information in the following way.
Even when a person appears to be sleeping quietly in bed, the body is always making slight movements. A sheet-type sensor detects not only larger movements such as turning over, but also subtle vibrations caused by the heartbeat and by the movement of the chest during breathing.
These vibrations are then converted into electrical signals.
The vibration signals that are collected contain multiple components, including heart rate, respiration, body movement, and noise such as snoring or sleep talking.
These signals are then separated by using differences in frequency bands and other characteristics, allowing the system to estimate heart rate, respiration, and body movement.
It also calculates phase coherence, an indicator that quantifies how consistently the rhythms of heartbeats and respiration are linked to each other.
The resulting data—heart rate, respiration, body movement, and phase coherence—are then input into a model that has been trained using sleep stages identified by polysomnography as teacher data.
Based on that model, the system determines five sleep stages: Wake, REM, N1, N2, and N3.
In other words, Suishin Delta works in the following way:
Place the sensor under the mattress
→ detect subtle vibrations in the mattress and extract signals such as heart rate and respiration
→ compare those signals with data that have already been accurately measured by polysomnography
→ estimate the person’s sleep state
As for aams+, the publicly available product information does not clearly explain its internal mechanism in detail.
However, because it is also a mat-type product that acquires vital signs and sleep-related data, it seems highly likely that it uses a similar basic principle—namely, estimating heart rate, respiration, and body movement from vibrations.
2) and 3) How Fall Risk Is Predicted: “Reha3.0”
What Is Reha3.0?
So far, we have looked at the general flow of how biometric information may be collected from a mat.
But how does the system go on to automatically estimate ADL indicators such as FIM and evaluate fall risk from there?
The key to steps 2 and 3 appears to be the AI fall prediction system Reha3.0, developed by Rehabilitation3.0 Co., Ltd. Since Reha3.0 is patented, we can use the patent description to look more closely at how the fall prediction mechanism works.
(Patent Application 2020-024812: Occupational Therapy Support Device, Artificial Intelligence Learning Device for an Occupational Therapy Support Device, and Method of Using an Occupational Therapy Support Device)
What Is FIM?
According to the Reha3.0 patent, the system has a function that:
takes objective sleep data and the person’s basic information as input, and uses AI to estimate and output FIM items, physical function, fall risk, and related indicators.
So first, it is helpful to clarify what FIM actually refers to.
FIM stands for Functional Independence Measure.
It is an assessment scale used to score activities of daily living (ADL) in terms of how much assistance a person requires in order to function independently.
It includes both motor items—such as transfers, mobility, and toileting—and cognitive items—such as comprehension, expression, social interaction, problem solving, and memory.
In other words, FIM is not simply an index of whether a person “can move” or “cannot move.”
It is a measure of how independently the person can perform daily activities and how much assistance is needed.
Estimating FIM
According to the Reha3.0 patent, the flow for estimating FIM items is as follows:
Input the necessary data
↓
The AI outputs estimated data based on that input
The two main types of input data are:
- Sleep-related data obtained from the mat
(such as the number of times the person turns over, the number of body movements, the number and timing of toilet visits, sleep/wake rhythm, respiration, and pulse rate) - Basic user information already known in advance
(such as age, height, weight, and medical history)
The “sleep data” here appear to be data automatically collected by sensors such as a mat-type device, rather than something entered manually.
Reha3.0 itself is also described as being able to work with multiple measurement devices rather than only one specific mat.
According to the patent, the AI then outputs estimated data such as:
- ADL data, including FIM items
- Physical function data, such as grip strength
- Fall risk, which is included as part of the ADL-related data
In this system, FIM is not scored directly by a human evaluator at that moment.
Instead, AI estimates it from objective data such as sleep patterns and basic personal information.
For that reason, the patent suggests that the system may reduce variation between evaluators and provide data that are easier to use in actual care.
That said, activities such as grooming, dressing, and eating are not directly linked to movement in bed, and subtle cognitive nuances cannot be directly measured by sensors alone.
Therefore, it seems likely that the AI estimates these factors indirectly as related conditions based on patterns learned from the combination of sleep data and basic information.
Displaying Fall Risk Based on Estimated ADL (FIM)
The patent also describes a mechanism in which fall risk is included within the ADL-related data.
In other words, the flow is:
Sleep data + basic information
→ AI estimates ADL and physical function
→ fall risk is also output as part of those results
The patent further states that, in order to improve accuracy, the following types of data may also be included as inputs:
- Environmental data during sleep, such as room temperature, humidity, and light level
- The person’s own subjective impressions, such as “I slept well”
- Past data history combined with time-related information
An article in the Silver Industry Newspaper described the system as making estimates “based on day-to-day changes.”
I believe this likely refers to the system’s ability to estimate risk using not only current data but also past history.
Practical Use in Care Settings
I have not personally used a monitoring sensor such as aams+ in practice, but I have been thinking about what kinds of benefits it could offer in care settings, how it might be used effectively, and in what situations I would want to try using it.
It May Reduce the Burden of Room Rounds
If each user’s movements can be displayed in real time in a single overview, the number of room visits required simply to check on residents may be reduced.
This could be especially helpful on night shift, when a small number of staff often need to monitor many people at once.
Being able to view the overall situation on a monitor and decide priorities accordingly would be a major advantage.
It may also help staff notice changes sooner and respond more quickly.
It May Support More Individualized Care by Making Sleep Patterns Visible
When sleep status can be seen more clearly, it may become easier to connect that information to individualized care.
Rather than deciding uniformly, for example, “diaper change at this time” or “toilet assistance at that time,” care may be provided in a way that matches each person’s own sleep and movement patterns.
If toileting care can be timed according to the person’s actual condition, it may become less disruptive to their sleep.
Providing care only when it is truly needed may reduce not only the burden on the user, but also the burden on staff.
The Displayed Fall Risk Should Be Treated as a Starting Point, Not the Final Judgment
When a fall-risk display or alert appears, I believe it is important to first confirm the person’s actual condition.
That is because while risk assessment itself may, to some extent, be performed similarly by a machine or by a human, what happens after that depends greatly on the individual person.
For example, if staff can recognize patterns such as, “When this alert appears, this resident often becomes restless around toileting time,” then it becomes possible to think in terms of:
the display + the person’s condition at that moment + the actual response taken
When those three are considered together, care may become easier to standardize across the team without relying too heavily on one individual staff member’s experience or intuition.
At the same time, simply making decisions based on the display alone would be dangerous and requires caution.
In fact, I myself have had experiences using a bed-exit sensor with a person with dementia, where the sensor went off frequently and the person’s behavior pattern gradually became familiar.
In that kind of situation, it becomes easy to assume, “This is probably a safe call,” and that kind of assumption can lead to accidents such as falls.
It May Also Be Helpful in End-of-Life Care or Sudden Changes in Condition
I also think this kind of system may be useful in end-of-life care or in situations where sudden deterioration is a concern.
In long-term care facilities, even when a resident is in the terminal stage or at risk of sudden deterioration, equipment such as ECG monitors is often not used in the way it would be in a hospital.
As a result, even when staff are watching closely, a person may sometimes be found only after breathing has already stopped, and it may be unclear when that change occurred.
If changes in respiration and body movement can be tracked more easily through this kind of system, it may provide reassurance not only to staff but also to the resident’s family.
Recorded Data May Also Help When Consulting Physicians
The fact that the data remain as a record also seems useful when consulting a physician.
This is especially valuable at night, when there are long periods that cannot be directly observed in detail.
Having objective information may make it easier to discuss adjustments to sleeping medication or responses to nighttime agitation.
In turn, that may help staff and physicians identify medications or care approaches that are better suited to the person’s actual condition.
Sensors Alone Cannot Capture Everything Related to Fall Risk
When it comes to fall risk, there are still many factors that cannot be fully captured by sensors alone.
For example, the environment around the bed, the person’s facial expression, their complaints, or a general sense that “something feels different from usual” are often things that become clear only when someone actually goes to the bedside and observes them directly.
That is exactly why I believe it is important to use sensor information together with on-site observation.
Points to Consider Before Introducing the System
Price
When considering whether to introduce a system like this, one of the first questions is price.
According to the manufacturer’s publicly available information, aams+ does not appear to have a single fixed listed price, so the actual cost would likely need to be confirmed directly with the seller.
As a reference point, the version without the fall-risk notification function, aams, is listed on a long-term care equipment distribution website with a suggested retail price of 178,000 yen as of February 2026.
Subsidy Programs
In recent years, the Japanese government has been promoting the introduction of care technology, and monitoring sensors may qualify for subsidy programs.
Support for introducing care technology is provided by local governments, and in some municipalities, for example, subsidies may cover up to 300,000 yen per monitoring device, as well as up to 7.5 million yen per facility for communication environment development.
However, the details of these programs vary depending on the timing and the municipality, so they need to be checked carefully.
Productivity Improvement Promotion System Add-On
In addition, if the operational structure after introduction is properly established, it may also be possible to qualify for the Productivity Improvement Promotion System Add-On (Levels I and II) under Japan’s long-term care reimbursement system.
According to materials from the Ministry of Health, Labour and Welfare, the requirements are not limited to introducing technology alone.
They also include ongoing efforts such as holding committee meetings, implementing safety measures, improving workflow, and submitting data.
Level I has stricter requirements than Level II and appears to require the use of multiple technologies as well as broader implementation efforts.
An add-on in this context means additional reimbursement points that can be claimed for services provided to users under the long-term care fee system.
In other words, if the requirements are met, the facility can receive additional reimbursement on top of the standard care fees.
Unlike a one-time subsidy at the time of introduction, this add-on can continue to be claimed unless there is a revision in the reimbursement system or the requirements change.
That means the financial benefit can accumulate over time.
When this is considered together with possible labor-cost savings from reduced workload and the value of being able to promote the facility’s efforts, it may make it easier to recover the initial cost of introduction.
Closing thoughts
The number of monitoring devices continues to grow year by year, but one of the distinctive features of aams+ is that it does not simply detect movement.
It also visualizes fall risk through AI.
However, information about “what benefits the system offers” may help spark interest, but it does not necessarily lead to successful use in practice.
If staff do not understand what kinds of information a sensor such as aams+ is using and how it visualizes risk, there is a danger of relying on the machine too heavily and allowing that to lead to accidents.
Or the system may be introduced, but not used effectively, with the result that the burden on staff does not actually decrease.
Even simply understanding that aams+ estimates risk through AI based on information such as body movement, heart rate, and respiration collected from the mat may make it easier to connect the technology with practical on-site judgment and to use the device as something that is truly useful.
Perhaps devices like this only become real partners for care staff once they are properly understood and used well.
I have not yet personally seen this kind of sensor introduced in facilities close to me, but as staffing shortages continue, I feel that systems like this may become increasingly common not only in long-term care settings, but also in hospitals.
On this blog, I mainly focus on how welfare equipment and medical products are actually received in care settings and in what kinds of situations they are most likely to provide value.
From the perspective of real healthcare and long-term care practice, I aim to share information that helps bridge the gap between companies, service providers, and the field.
Based on that perspective, I offer support in areas such as explaining medical materials and care products, writing technical articles, reviewing products, and assisting with market development by drawing on both my clinical nursing experience and my understanding of patents. →Services
For inquiries about explanatory articles, product reviews, promotional and communication support, or exhibition-related assistance, please feel free to contact me through the form on this blog.
Disclaimer: The content of this article is provided for reference purposes only and does not guarantee accuracy.
Any decision to purchase or use a product should be made at your own discretion and responsibility.
References
- Silver Industry Newspaper, February 10, 2026 issue: “aams+ Equipped with AI-Based Fall Prediction Function”
- Patent No. 7301275: Sleep State Estimation System
- Patent Application 2020-024812: Occupational Therapy Support Device, Artificial Intelligence Learning Device for an Occupational Therapy Support Device, and Method of Using an Occupational Therapy Support Device
- Biosilver Co., Ltd. https://www.biosilver.co.jp/products/products-410/
- Rehabilitation3.0 Co., Ltd. https://rehabilitation3.jp/
- Ministry of Health, Labour and Welfare https://www.mhlw.go.jp/content/001238432.pdf
- Kaientai https://www.kaientai.cc/goods.aspx?webcd=516676&utm_source=chatgpt.com